
Abstract
Background
Acute healthcare utilization attributed to alcohol use disorders (AUD) and other substance use disorders (SUD) is rising.
Objective
To describe the prevalence and characteristics of emergency department (ED) visits and hospitalizations made by adults with AUD or SUD.
Design, Setting, and Participants
Observational study with retrospective analysis of the National Hospital Ambulatory Medical Care Survey (2014 to 2018), a nationally representative survey of acute care visits with information on the presence of AUD or SUD abstracted from the medical chart.
Main Measures
Outcome measured as the presence of AUD or SUD.
Key Results
From 2014 to 2018, the annual average prevalence of AUD or SUD was 9.4% of ED visits (9.3 million visits) and 11.9% hospitalizations (1.4 million hospitalizations). Both estimates increased over time (30% and 57% relative increase for ED visits and hospitalizations, respectively, from 2014 to 2018). ED visits and hospitalizations from individuals with AUD or SUD, compared to individuals with neither AUD nor SUD, had higher percentages of Medicaid insurance (ED visits: AUD: 33.1%, SUD: 35.0%, neither: 24.4%; hospitalizations: AUD: 30.7%, SUD: 36.3%, neither: 14.8%); homelessness (ED visits: AUD: 6.2%, SUD 4.4%, neither 0.4%; hospitalizations: AUD: 5.9%, SUD 7.3%, neither: 0.4%); coexisting depression (ED visits: AUD: 26.3%, SUD 24.7%, neither 10.5%; hospitalizations: AUD: 33.5%, SUD 35.3%, neither: 13.9%); and injury/trauma (ED visits: AUD: 51.3%, SUD 36.3%, neither: 26.4%; hospitalizations: AUD: 31.8%, SUD: 23.8%, neither: 15.0%).
Conclusions
In this nationally representative study, 1 in 11 ED visits and 1 in 9 hospitalizations were made by adults with AUD or SUD, and both increased over time. These estimates are higher or similar than previous national estimates using claims data. This highlights the importance of identifying opportunities to address AUD and SUD in acute care settings in tandem with other medical concerns, particularly among visits presenting with injury, trauma, or coexisting depression.
Similar content being viewed by others
INTRODUCTION
Deaths from alcohol use disorder (AUD) and other substance use disorders (SUD) are at an all-time high in the United States (US), with an estimated 93,000 deaths attributed to alcohol-related harms annually1 and over 93,000 deaths from drug overdose deaths in 2020.2, 3 Acute care visits, including emergency department (ED) visits and hospitalizations, related to AUD or SUD (herein abbreviated AUD/SUD) are increasing and represent opportunities to engage individuals in substance use care.4,5,6 Individuals with untreated AUD/SUD are more likely to access acute care services due to higher rates of motor vehicle accidents, interpersonal violence, and presentations for intoxication or overdose.7,8,9 Many are motivated to reduce use during acute care visits; nonetheless, rates of AUD/SUD treatment initiation and post-discharge referrals for outpatient treatment remain low in these settings, in part, potentially due to low rates of engagement in post-discharge AUD/SUD treatment.9,10,11 Efforts are needed to examine and thus improve structures for successful treatment engagement.
Undertreatment of AUD/SUD in the ED and hospital may be largely due to underrecognized prevalence. National findings from the Healthcare Cost and Utilization Project Nationwide Emergency Department Sample (HCUP-NEDS) found a 4% prevalence of AUD/SUD among ED visits in 2017, and HCUP National Inpatient Sample (HCUP-NIS) data suggest a 10% prevalence of AUD/SUD among hospitalizations in 2016 and 2017.12, 13 However, these estimates rely exclusively on billing diagnoses to identify individuals with AUD/SUD, which may underestimate the true prevalence of these conditions.14, 15 Acute care providers may be underdiagnosing AUD/SUD if the reasons for visits are not directly related.7, 14, 16
Understanding the prevalence of AUD/SUD in acute care settings and associations with psychosocial and medical characteristics could help policymakers and health system leaders allocate resources and improve acute care addiction services.10, 11 Thus, we sought to estimate the national prevalence, trends, and characteristics of AUD/SUD visits in acute care settings using a nationally representative dataset with unique information on AUD and SUD comorbidities. We also compared differences in characteristics of acute care visits by safety-net status to assess for potential differential prevalence in under-resourced settings.
METHODS
Study Design, Setting, and Population
We conducted a retrospective analysis of 2014–2018 data from the National Hospital Ambulatory Medical Care Survey (NHAMCS), an annual national dataset representative of ED visits and resulting hospitalizations.17 NHAMCS is administered annually by the National Center for Health Statistics (NCHS). Each year, NCHS develops the NHAMCS data collection form, defining variables for medical chart abstraction, which is then reviewed by an expert panel for additions, deletions, and modifications approximately every two years.17 Trained staff abstract visit data from the medical chart with NCHS oversight. Using a multi-stage probability sampling design, the NHAMCS dataset captures a representative sample of all visits to non-federal, general, short-stay acute care hospitals in the US.17, 18 The strengths of NHAMCS include its rigorous statistical methodology in creating a nationally representative sample, a wide array of variables collected annually, and the ability to examine longitudinal trends when multiple years are combined.
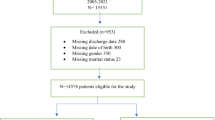
Since 2014, NHAMCS has collected data on AUD (“alcohol misuse, abuse, or dependence”) and SUD (“substance abuse or dependence”) as comorbidities professionally abstracted from the medical chart regardless of the reason for visit or associated medical billing codes; 2018 is the most recent year for which data are publicly available. We included all ED visits and hospitalizations resulting from an ED visit made by individuals aged 18 years or older. We excluded repeat visits to the same hospital within the past 72 h and those that were a follow-up ED visit to minimize repeat visits and to best approximate the prevalence of unique individuals with AUD/SUD accessing acute care services.
Primary Outcome
The primary measure of interest was whether the ED visit or hospitalization was made by an individual with AUD/SUD. Per NHAMCS, trained staff ascertained the presence of AUD/SUD based on review of all available medical chart data, including ED and non-ED physician notes, laboratory/imaging results, and diagnostic codes related to current/prior visits. NHAMCS defines the presence of these conditions as presence of any of the following: (1) mention of AUD, SUD, or related diagnoses in the chart (including opioid use disorder); (2) alcohol- or substance use–related ICD visit diagnoses (AUD: ICD-9 305.00–305.93, ICD-10 F10; SUD: ICD-9 codes 304.00–30.493, 292, 291, ICD-10 F11-16, F18, F19); (3) specific AUD/SUD terms in medical records that suggest potential presence of AUD/SUD (AUD: “alcoholism,” “excessive alcohol use,” “heavy drinking,” “problem drinking,” “binge drinking,” or “chronic drinking;” SUD: “addiction,” “addict,” “illicit drug use,” “injection/intravenous drug use/user (IDU, IVDU, IVDA),” “drugged,” “stoned,” or “high;” or 4) for SUD, if specific unlawful drug use is noted (e.g., cocaine or methamphetamine use). SUD did not include tobacco/nicotine or alcohol use.19, 20 NHAMCS does not characterize SUD subtypes (e.g., opioids vs. stimulants). AUD and SUD comorbidities are not mutually exclusive.
Prevalence, Trends, and Characteristics
We estimated the prevalence and number of ED visits and hospitalizations from 2014 to 2018 made by individuals with AUD/SUD, AUD only, and SUD only. We compared the average annual percentage of visits made by individuals with AUD (i.e., “AUD ED visits” and “AUD hospitalizations”) and SUD (i.e., “SUD ED visits,” and “SUD hospitalizations”) with visits made by individuals with neither disorder (i.e., “non-AUD/SUD ED visits” or “non-AUD/SUD hospitalizations”). We assessed hospital, demographic, and clinical characteristics of ED visits and hospitalizations. We used the imputed measure of race/ethnicity provided by NHAMCS accounting for the 16–18% of missing race/ethnicity data.21 We defined experiencing homelessness as residence listed as “homeless/homeless shelter.” We defined multimorbidity as the presence of two or more comorbidities assessed by NHAMCS (including Alzheimer’s dementia, asthma, cancer, cerebrovascular disease, chronic obstructive pulmonary disease, coronary artery disease, depression, diabetes, chronic kidney disease, end-stage renal disease, venous thromboembolism, HIV/AIDS, hypertension, obesity, obstructive sleep apnea, and osteoporosis, and excluding alcohol and substance use disorders).22
We included NHAMCS measures of whether visits were related to injury/trauma or overdose/poisoning; had a non-psychiatric mental health evaluation (NHAMCS defines a non-psychiatric mental health evaluation as any evaluation done by a social worker, psychologist, or counselor providing mental health services, but excluding psychiatrists)19, 20; and disposition status. We defined “self-directed discharge” as any discharge where the patient was documented as “left without being seen,” “left against medical advice,” or “left before treatment complete.” We evaluated the most common reasons for visit.
Safety-Net Hospitals
For AUD visits and SUD visits, we stratified analyses by comparing differences in characteristics between safety-net and non-safety-net settings. We defined safety-net status using the approach employed by NCHS: a hospital with either more than 30% of visits with Medicaid as expected source of payment, more than 30% of visits uninsured, or a combined Medicaid and uninsured percentage greater than 40%.23 We hypothesized safety-net AUD and SUD acute care visits would have a greater prevalence of markers of social disadvantage and greater clinical severity compared to non-safety-net hospitals.
Statistical Analyses
We used linear regression with visit year as an ordinal predictor to test for trends over time. For all other analyses, we combined data across all study years and reported estimated annual averages. Bivariate analyses assessed demographic, hospital, and visit characteristics comparing AUD visits or SUD visits versus non-AUD/SUD visits, using Pearson chi-square testing for categorical variables and bivariate linear regression for continuous variables. We defined statistical significance as p value <0.05. All analyses accounted for the complex survey design and used visit, strata, and primary sampling unit design weights provided by NHAMCS to reflect national estimates. We conducted analyses using Stata LP 16.0 (StataCorp, College Station, TX). We noted when reported national estimates were not considered robust per NCHS, including analyses with an unweighted count of less than 30 visits and/or a standard error ≥30% of the weighted estimate.17, 18 The University of California, San Francisco Institutional Review Board exempted this study from review.
RESULTS
Prevalence and Trends in AUD and SUD Among ED Visits and Hospitalizations
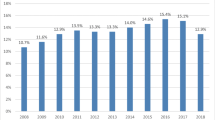
From 2014 to 2018, acute care visits made by individuals with AUD/SUD accounted for an annual average of 9.4% of ED visits (9.3 million ED visits) and 11.9% of hospitalizations (1.4 million hospitalizations) (Fig. 1, Appendix 1). AUD/SUD ED visits and hospitalizations increased significantly over time: from 8.0% of annual ED visits in 2014 to 10.4% 2018 (a relative increase of approximately 30% [p=0.04]), and 9.2% of hospitalizations in 2014 to 14.4% in 2018 (a relative increase of approximately 57% [p<0.001]). AUD visits accounted for an annual average of 3.8% of all ED visits (range 3.4–4.0%) and 5.8% of hospitalizations (range 4.1–7.3%). SUD visits accounted for an annual average of 7.3% of ED visits (range 6.1–8.3%) and 8.0% of hospitalizations (range 6.3–9.7%).

National Prevalence of Alcohol Use Disorder (AUD) and/or other substance use disorders (SUD) among adult emergency department visits and hospitalizations. Data source: National Hospital Ambulatory Medical Care Survey. Weighted average annual number of emergency department visits and hospitalizations for individuals with AUD/SUD from 2014 to 2018 were 9,284,400 and 1,362,600, respectively. Both ED visits and hospitalizations made by individuals with AUD/SUD increased significantly over time (AUD/SUD ED visits: p=0.04, AUD/SUD Hospitalizations: p<0.001 for trend). Visits by individuals with AUD/SUD include visits made by individuals with AUD, SUD, or both conditions.
AUD and SUD ED Visit Characteristics
Compared to non-AUD/SUD ED visits, both AUD ED visits and SUD ED visits had higher percentages of individuals with male sex, experiencing homelessness, and Medicaid insurance (Table 1). AUD ED visits were more common among individuals 45–64 years old, while SUD ED visits were more common among individuals 18–44 years old. Race/ethnicity was similar across all groups.
Regarding clinical characteristics, both AUD ED visits and SUD ED visits were associated with coexisting depression (AUD: 26.3%, SUD 24.7%, neither 10.5%, p<0.001 for both comparisons) and HIV/AIDS; presented much more commonly for injury/trauma (AUD: 51.3%, SUD: 36.3%, neither: 26.4%, p<0.001 for both comparisons) and overdose/poisoning (AUD: 5.4%, SUD: 7.7%, neither: 3.3%); and were more likely to receive non-psychiatric mental health evaluations (AUD: 8.3%, SUD: 6.3%, neither: 1.1%; p<0.001 for both comparisons).
For disposition, both AUD ED visits and SUD ED visits more commonly resulted in transfers to a psychiatric hospital (AUD: 3.3%, SUD: 3.3%, neither: 0.6%, p<0.001 for both); self-directed discharge (AUD: 2.9%, SUD: 2.8%, neither 2.1%, p=0.04 for AUD, p=0.004 for SUD); and inpatient admission (AUD: 17.9%, SUD: 12.8%, neither: 11.1%; p<0.001 for AUD, p=0.04 for SUD).
The most common reasons for AUD ED visits were alcohol related (27.4% collectively) and differed from non-AUD/SUD ED visits (Table 2). In contrast, the most common reasons for SUD ED visits were similar to non-AUD/SUD ED visits, except for “other symptoms of psychosis” (9.2% of SUD ED visits), adverse effects of alcohol (8.9%), and adverse effects of drug use (7.5%).
AUD and SUD Hospitalization Characteristics
Comparisons for AUD hospitalizations and SUD hospitalizations versus non-AUD/SUD hospitalized paralleled earlier findings of ED visits for most characteristics (Table 3). Unlike ED visits, AUD hospitalizations and SUD hospitalizations were not significantly different in urban hospital status, region, or hospital safety net status compared to non-AUD/SUD hospitalizations. AUD hospitalizations and SUD hospitalizations also more commonly presented with injury/trauma than non-AUD/SUD hospitalizations (AUD: 31.8%, SUD: 23.8%, neither: 15.0%, p<0.001 for both), though only SUD hospitalizations had significantly higher percentages of overdose/poisoning. AUD hospitalizations and SUD hospitalizations were markedly more associated with admission to an inpatient mental health or detoxification facility within that hospital (AUD: 18.3%, SUD: 19.2%, neither: 1.8%; p<0.001 for both comparisons). The length of stay was similar across groups. Admitting diagnoses were similar, though unweighted counts were too small to calculate robust national estimates (Appendix 2).
Differences Between AUD and SUD ED Visits and Hospitalizations by Safety-Net Status
The proportion of AUD and SUD acute care visits in safety-net settings was similar to non-AUD/SUD visits (Tables 1 and 3). Across safety-net settings, non-safety-net AUD ED visits were comparable to safety-net AUD ED visits. Safety-net AUD ED visits had higher percentages of racial/ethnic minority status; Medicaid insurance; Midwest and West regions; and lower percentages of with inpatient admission than non-safety-net AUD ED visits (Table 4). Meanwhile, safety-net SUD ED visits had higher involvement of injury/trauma than non-safety-net SUD ED visits (safety-net: 39.6%, non-safety-net: 33.9%; p=0.02) and lower involvement of overdose/poisoning (safety-net: 6.5%, non-safety-net: 8.6%; p=0.05). Among AUD hospitalizations and SUD hospitalizations, safety-net settings were also similar to non-safety net hospitalizations in most characteristics, though sample sizes for several characteristics were too small to reliably estimate (Appendix 3).
DISCUSSION
In this nationally representative study, AUD/SUD was present in about 1 of 11 ED visits and 1 of 9 hospitalizations in the US annually between 2014 and 2018, and both increased over time (30% and 57% relative increase from 2014 to 2018 for ED visits and hospitalizations, respectively, p<0.05). Both AUD acute care visits and SUD acute care visits were more likely to be associated with markers of social disadvantage (e.g., Medicaid insurance, experiencing homelessness), coexisting depression, presentations for injury/trauma, and mental health service utilization (including increased non-psychiatric mental health evaluations, and admissions to mental health and detoxification facilities). Finally, the proportion of AUD visits and SUD visits in safety-net settings was similar to non-AUD/SUD visits, with similar visit characteristics between safety-net and non-safety-net hospitals.
Our estimated 9.4% prevalence of AUD/SUD among ED visits is higher than a recent study’s estimate of 4% using HCUP-NEDS data from 2017.13 This discrepancy is potentially attributed to differences in measuring SUD in NHAMCS compared to HCUP-NEDS, as our 4% estimate of AUD among ED visits is the same as another study using HCUP-NEDS data from 2013.6 Our study is the first to use nationally representative NHAMCS data with ascertainment of AUD/SUD through comprehensive medical chart review, rather than relying solely on billing diagnosis codes from claims data commonly used in other studies and national datasets. Comprehensive chart review data are more likely to reflect true prevalence compared to using diagnoses codes, though capturing episodes of heavy use or misuse as potential alcohol or other substance use disorders may result in some overestimates.15 Additionally, capturing the use of stigmatizing terms like “addict” may reflect provider bias rather than an accurate diagnosis of use disorders.24 On the other hand, it is also possible this method may underestimate true AUD/SUD prevalence by relying on clinician recognition and documentation of signs and symptoms in the medical chart. Prior studies have found acute care physicians underrecognize and underdiagnose AUD/SUD conditions when compared to universal diagnostic screening and assessment using the Diagnostic and Statistical Manual of Mental Disorders 5th-edition (DSM-5) criteria.14, 25
Meanwhile, our estimate of AUD/SUD being associated with 11.9% of hospitalizations is similar to the 10% found in other studies using HCUP-NIS data from 2016 and 2017.12, 13 Single-center studies in urban centers implementing universal screening for potential AUD/SUD have found even higher estimates of 16–21%, suggesting estimates may be even higher in populations at risk for AUD/SUD.14, 16, 26 Our estimated prevalence of AUD/SUD among hospital visits was comparable to those of other common coexisting chronic medical conditions, including congestive heart failure (CHF) (15% of hospitalizations). Though health care systems are equipped to diagnose and treat these other similarly prevalent chronic medical conditions, the same is not true for AUD/SUD. Both evidence-based pharmacotherapies for AUD/SUD and referrals to specialty substance use treatment on discharge remain underutilized, in part potentially due to lack of training for clinicians and limited capacity of inpatient behavioral health staff.10, 11, 27, 28
We found that estimated AUD/SUD prevalence among ED visits and hospitalizations increased over time, mirroring trends observed in other national and statewide studies of both community-based and acute care cohorts.4, 29,30,31,32 AUD acute care visits and SUD acute care visits were more common among individuals with coexisting depression and required more non-psychiatric mental health evaluations, consistent with prior studies finding individuals with coexisting psychiatric and AUD/SUD are more likely to access acute care services.33,34,35,36 Despite the relationship between AUD/SUD and psychiatric illness, inpatient behavioral treatment and access to dual mental health and addiction treatment services after discharge are largely unavailable and underfunded nationwide.37 Our finding of AUD acute care visits and SUD acute care visits being highly associated with Medicaid insurance raises further concern. Accessing addiction services can be challenging for Medicaid populations, in part due to lack of standardization for outpatient treatment and reimbursement of inpatient addiction treatment.27, 37 An important policy intervention would be standardizing Medicaid coverage for AUD/SUD treatment across states, given the patchwork of AUD/SUD Medicaid treatment coverage that is currently in place, as well as bolstering mental health and behavioral treatment services within health networks.27, 37
Contrary to our hypothesis, both AUD acute care visits and SUD acute care visits were similar across a range of characteristics between safety-net and non-safety-net settings, including experiencing homelessness, depression, and multimorbidity. While individuals with AUD or SUD have historically been viewed as “safety net populations,” our findings show the impact of addiction disorders irrespective of safety-net status, highlighting the need to prioritize AUD and SUD care across all types of health systems.
Our findings highlight several opportunities for intervention. First, given the high prevalence of AUD/SUD in acute care settings, there is an urgency to develop interventions that allow health care systems to treat these conditions. Although best practice evidence is still emerging from acute care settings, potential interventions include hospital-based addiction consult services; training ED and hospital providers to initiate pharmacotherapy for AUD/SUD as part of routine care; and supporting AUD/SUD-related social work and/or patient navigation services for linkages to post-discharge AUD/SUD specialty care.27, 38,39,40,41 Second, the high incidence with which AUD/SUD ED visits and hospitalizations presented with trauma/injury was striking. Although mandated screening for AUD at Level I trauma centers exists, no such mandate exists for SUD screening.42 These findings highlight the potential implications for implementing systems of screening, assessment, and treatment for AUD/SUD in trauma settings.43
Our study had several limitations. First, our study data does not include data after 2018, although the trends we identified and early analyses of AUD/SUD data during the COVID-19 pandemic suggest that the prevalence of AUD/SUD may have markedly increased in the intervening years.44,45,46,47 Second, NHAMCS does not distinguish between severity or type of SUD. Understanding drug type has important implications in identifying SUD treatment gaps and further tailor interventions in acute care settings.
AUD/SUD are common and increasing in prevalence among individuals with acute care visits in the USA. Individuals with AUD/SUD accessing acute care visits more commonly: had Medicaid, coexisting depression, were experiencing homelessness, received mental health service utilization; and presented with injury and trauma. As morbidity and mortality from AUD/SUD increase, ED and hospitals, regardless of safety-net status, must be ready and equipped to provide hospital-based and post-discharge AUD/SUD treatment to bend the curve on the epidemic of alcohol- and other substance use–related deaths.
References
Esser MB. Deaths and Years of Potential Life Lost From Excessive Alcohol Use — United States, 2011–2015. MMWR Morb Mortal Wkly Rep. 2020;69. https://doi.org/10.15585/mmwr.mm6930a1
Ahmad FB, Rossen LM, Sutton P. Provisional Drug Overdose Death Counts. National Center for Health Statistics.; 2021. Accessed June 30, 2021. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
American Medical Association Opioid Task Force. Opioid Task Force Report 2020: Physicians’ Progress toward Ending the Nation’s Drug Overdose and Death Epidemic; 2020. Accessed July 24, 2020. https://www.ama-assn.org/system/files/2020-07/opioid-task-force-progress-report.pdf
Weiss AJ, Bailey MK, O’Malley L, Barrett ML, Elixhauser A, Steiner CA. Opioid-Related Inpatient Stays and Emergency Department Visits by State, 2009–2014: Statistical Brief #21. Agency for Healthcare Research and Quality; 2017:16.
Mullins PM, Mazer-Amirshahi M, Pines JM. Alcohol-Related Visits to US Emergency Departments, 2001–2011. Alcohol Alcohol. 2017;52(1):119-125. https://doi.org/10.1093/alcalc/agw074
National Institute of Alcohol Abuse and Alcoholism. Alcohol-Related Emergency Department Visits and Hospitalizations and Their Co-Occurring Drug-Related, Mental Health, and Injury Conditions in the United States: Findings from the 2006-2010 Nationwide Emergency Department Sample (NEDS) and the Nationwide Inpatient Sample (NIS). In: Alcohol Epidemiologic Data Reference Manual. Vol 9. NIH Publications.; 2013.
Hawk K, D’Onofrio G. Emergency department screening and interventions for substance use disorders. Addiction Science & Clinical Practice. 2018;13(1):18. https://doi.org/10.1186/s13722-018-0117-1
Macias Konstantopoulos WL, Dreifuss JA, McDermott KA, et al. Identifying Patients With Problematic Drug Use in the Emergency Department: Results of a Multisite Study. Annals of Emergency Medicine. 2014;64(5):516-525. https://doi.org/10.1016/j.annemergmed.2014.05.012
Englander H, Dobbertin K, Lind BK, et al. Inpatient Addiction Medicine Consultation and Post-Hospital Substance Use Disorder Treatment Engagement: a Propensity-Matched Analysis. Journal of General Internal Medicine. Published online August 13, 2019. https://doi.org/10.1007/s11606-019-05251-9
Naeger S, Mutter R, Ali MM, Mark T, Hughey L. Post-Discharge Treatment Engagement Among Patients with an Opioid-Use Disorder. J Subst Abuse Treat. 2016;69:64-71. https://doi.org/10.1016/j.jsat.2016.07.004
Rosenthal ES, Karchmer AW, Theisen-Toupal J, Castillo RA, Rowley CF. Suboptimal Addiction Interventions for Patients Hospitalized with Injection Drug Use-Associated Infective Endocarditis. Am J Med. 2016;129(5):481-485. https://doi.org/10.1016/j.amjmed.2015.09.024
Owens PL, McDermott KW, Heslin KC. Inpatient Stays Involving Mental and Substance Use Disorders, 2016. Agency for Healthcare Research and Quality; 2019. www.hcup-us.ahrq.gov/reports/statbriefs/sb249-Mental-Substance-Use-Disorder-Hospital-Stays-2016.pdf
Peterson C, Li M, Xu L, Mikosz CA, Luo F. Assessment of Annual Cost of Substance Use Disorder in US Hospitals. JAMA Netw Open. 2021;4(3):e210242. https://doi.org/10.1001/jamanetworkopen.2021.0242
Wakeman SE, Herman G, Wilens TE, Regan S. The prevalence of unhealthy alcohol and drug use among inpatients in a general hospital. Substance Abuse. Published online August 2019:1-9. https://doi.org/10.1080/08897077.2019.1635961
Asao K, McEwen LN, Lee JM, Herman WH. Ascertainment of outpatient visits by patients with diabetes: The National Ambulatory Medical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS). Journal of Diabetes and its Complications. 2015;29(5):650-658. https://doi.org/10.1016/j.jdiacomp.2015.03.019
Brown RL, Leonard T, Saunders LA, Papasouliotis O. The Prevalence and Detection of Substance Use Disorders among Inpatients Ages 18 to 49: An Opportunity for Prevention. Preventive Medicine. 1998;27(1):101-110. https://doi.org/10.1006/pmed.1997.0250
McCaig LF, Burt CW. Understanding and Interpreting the National Hospital Ambulatory Medical Care Survey: Key Questions and Answers. Annals of Emergency Medicine. 2012;60(6):716-721.e1. https://doi.org/10.1016/j.annemergmed.2012.07.010
Centers for Disease Control and Prevention. NAMCS/NHAMCS - Scope and Sample Design; 2019. Accessed April 14, 2020. https://www.cdc.gov/nchs/ahcd/ahcd_scope.htm
National Center for Health Statistics. 2014 NHAMCS Micro-Data File Documentation. National Center for Health Statistics; 2014. Accessed April 14, 2020. https://data.nber.org/nhamcs/docs/nhamcsed2014.pdf
National Center for Health Statistics. 2015 NHAMCS Micro-Data File Documentation.; 2015.
Centers for Disease Control and Prevention. NAMCS/NHAMCS - Estimation Procedures.; 2019. Accessed April 14, 2020. https://www.cdc.gov/nchs/ahcd/ahcd_estimation_procedures.htm
Navickas R, Petric V-K, Feigl AB, Seychell M. Multimorbidity: What do we know? What should we do? J Comorb. 2016;6(1):4-11. https://doi.org/10.15256/joc.2016.6.72
Burt C, Arispe I. Characteristics of Emergency Departments Serving High Volumes of Safety-Net Patients: United States, 2000. National Center for Health Statistics; 2004.
van Boekel LC, Brouwers EPM, van Weeghel J, Garretsen HFL. Stigma among health professionals toward patients with substance use disorders and its consequences for healthcare delivery: Systematic review. Drug and Alcohol Dependence. 2013;131(1):23-35. https://doi.org/10.1016/j.drugalcdep.2013.02.018
Bernstein SL, D’Onofrio G. A Promising Approach For Emergency Departments To Care For Patients With Substance Use And Behavioral Disorders. Health Affairs. 2013;32(12):2122-2128. https://doi.org/10.1377/hlthaff.2013.0664
Walley AY, Paasche-Orlow M, Lee EC, et al. Acute Care Hospital Utilization Among Medical Inpatients Discharged With a Substance Use Disorder Diagnosis. Journal of Addiction Medicine. 2012;6(1):50-56. https://doi.org/10.1097/ADM.0b013e318231de51
Priest KC, McCarty D. The Role of the Hospital in the 21st Century Opioid Overdose Epidemic: The Addiction Medicine Consult Service. J Addict Med. 2019;13(2):104-112. https://doi.org/10.1097/ADM.0000000000000496
Substance Abuse and Mental Health Services Administration. Behavioral Health Workforce Report; 2020. Accessed December 28, 2020. https://www.samhsa.gov/sites/default/files/behavioral-health-workforce-report.pdf
Holland KM, Jones C, Vivolo-Kantor AM, et al. Trends in US Emergency Department Visits for Mental Health, Overdose, and Violence Outcomes Before and During the COVID-19 Pandemic. JAMA Psychiatry. Published online 2021:8.
California Health Care Foundation S. Substance Use in California: A Look at Addiction and Treatment. California Health Care Foundation; 2018. Accessed June 18, 2021. https://www.chcf.org/wpcontent/uploads/2018/09/SubstanceUseDisorderAlmanac2018.pdf
Grant BF, Chou SP, Saha TD, et al. Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV Alcohol Use Disorder in the United States, 2001-2002 to 2012-2013: Results From the National Epidemiologic Survey on Alcohol and Related Conditions. JAMA Psychiatry. 2017;74(9):911. https://doi.org/10.1001/jamapsychiatry.2017.2161
Grant BF, Saha TD, Ruan WJ, et al. Epidemiology of DSM-5 Drug Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions-III. JAMA Psychiatry. 2016;73(1):39-47. https://doi.org/10.1001/jamapsychiatry.2015.2132
Kêdoté MN, Brousselle A, Champagne F. Use of health care services by patients with co-occurring severe mental illness and substance use disorders. Mental Health and Substance Use. 2008;1(3):216-227. https://doi.org/10.1080/17523280802274886
Stewart SH. Alcoholics in Acute Medical Settings Have Increased Risk for other Drug, Mood, and Personality Disorders. Int J Psychiatry Med. 2007;37(1):59-67. https://doi.org/10.2190/E075-04TK-2N6J-1RH5
Curran GM, Sullivan G, Williams K, et al. Emergency department use of persons with comorbid psychiatric and substance abuse disorders. Annals of Emergency Medicine. 2003;41(5):659-667. https://doi.org/10.1067/mem.2003.154
Huynh C, Ferland F, Blanchette-Martin N, Ménard J-M, Fleury M-J. Factors Influencing the Frequency of Emergency Department Utilization by Individuals with Substance Use Disorders. Psychiatr Q. 2016;87(4):713-728. https://doi.org/10.1007/s11126-016-9422-6
Grogan CM, Andrews C, Abraham A, et al. Survey Highlights Differences In Medicaid Coverage For Substance Use Treatment And Opioid Use Disorder Medications. Health Affairs. 2016;35(12):2289-2296. https://doi.org/10.1377/hlthaff.2016.0623
Priest KC, Englander H, McCarty D. “Now hospital leaders are paying attention”: A qualitative study of internal and external factors influencing addiction consult services. J Subst Abuse Treat. 2020;110:59-65. https://doi.org/10.1016/j.jsat.2019.12.003
Trowbridge P, Weinstein ZM, Kerensky T, et al. Addiction consultation services - Linking hospitalized patients to outpatient addiction treatment. J Subst Abuse Treat. 2017;79:1-5. https://doi.org/10.1016/j.jsat.2017.05.007
Weinstein ZM, Wakeman SE, Nolan S. Inpatient Addiction Consult Service: Expertise for Hospitalized Patients with Complex Addiction Problems. Med Clin North Am. 2018;102(4):587-601. https://doi.org/10.1016/j.mcna.2018.03.001
Wakeman SE, Metlay JP, Chang Y, Herman GE, Rigotti NA. Inpatient Addiction Consultation for Hospitalized Patients Increases Post-Discharge Abstinence and Reduces Addiction Severity. J Gen Intern Med. 2017;32(8):909-916. https://doi.org/10.1007/s11606-017-4077-z
American College of Surgeons Committee on Trauma. Resources for the Optimal Care of the Injured Patient. American College of Surgeons Committee on Trauma; 2006.
Bongiovanni T, Hernandez S, Ledesma Y, et al. Surviving traumatic injury, only to die of acute drug poisoning: Should trauma centers be a path for intervention? Surgery. Published online April 15, 2021:S0039-6060(21) 00195-1. https://doi.org/10.1016/j.surg.2021.03.003
Blaney-Koen D. Issue Brief: Reports of Increases in Opioid-Related Overdose and Other Concerns during COVID Pandemic. American Medical Association; 2020. Accessed Aug. 24, 2020. https://www.ama-assn.org/system/files/2020-08/issuebrief-increases-in-opioid-related-overdose.pdf
McKay D, Asmundson GJG. COVID-19 stress and substance use: Current issues and future preparations. J Anxiety Disord. 2020;74:102274. https://doi.org/10.1016/j.janxdis.2020.102274
Spagnolo PA, Montemitro C, Leggio L. New Challenges in Addiction Medicine: COVID-19 Infection in Patients With Alcohol and Substance Use Disorders—The Perfect Storm. AJP. 2020;177(9):805-807. https://doi.org/10.1176/appi.ajp.2020.20040417
Drug Abuse Warning Network. DAWN and COVID-19. Substance Abuse and Mental Health Services Administration; 2020. Accessed Dec. 28, 2020. https://www.samhsa.gov/data/report/dawn-covid-19-profile
Acknowledgements
Contributors
We would like to thank Ms. Susan Schappert and Dr. Iris Shimizu from the National Center for Health Statistics for their correspondence and advice.
Funding
This study was supported by the National Heart, Lung and Blood Institute (R38 HL143581, Suen and K23 HL133441, Nguyen). The funding agency had no role in study design, data collection, analysis, the decision to publish, or the preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 33 kb)
Rights and permissions
About this article

Cite this article
Suen, L.W., Makam, A.N., Snyder, H.R. et al. National Prevalence of Alcohol and Other Substance Use Disorders Among Emergency Department Visits and Hospitalizations: NHAMCS 2014–2018. J GEN INTERN MED 37, 2420–2428 (2022). https://doi.org/10.1007/s11606-021-07069-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-021-07069-w